Happy New Year everybody and welcome back to worky blogging after the holiday fripperies of the last couple of weeks.
Yesterday Hafal’s management team met to look at the year ahead and the picture looks reasonably good notwithstanding the current squeeze. We certainly have several new developments confirmed not least from European funding and our substantial new Haverfordwest housing service is coming on-stream right now.
Meanwhile this is a good moment to remind ourselves what the key issues are for 2011 and beyond. I suggest the big five are as follows ...
(1) The Assembly ElectionHafal has an excellent track record of getting mental health onto politicians’ agendas at election time and we need to repeat that as the May election date draws near. The main lever in this game is to get parties and individual candidates to recognise that
there are votes in mental health, in other words many voters will be interested in what they have to say about care and treatment for people with a mental illness because they or their family or friends are personally affected.
The problem is often the extent to which voters are prepared to raise the issues in the first place (because of stigma or lack of confidence in articulating their concern) and that’s where Hafal can help. We will publish not just a manifesto but also guidance for voters on how to raise issues not least covering the four matters listed below ...
(2) Public ExpenditureWe are already actively engaged in the issues arising from the current squeeze having welcomed the Assembly Government’s declared commitment to protect mental health services and the priority placed on secondary health services and on protecting social care services for vulnerable people.
All good stuff but what guarantee is there that the NHS Local Health Boards and the Councils will put this into action? Our plan is to look for support from key players including Assembly Members, local councillors, and (importantly) the “insiders” who will want to protect services for which they have responsibility. We are particularly keen to encourage the non-executive Deputy Chairs of the LHBs (who have a brief for mental health services) to take care that LHB Chiefs and Directors of Finance don’t raid funding which should go to mental health.
In the same vein we also need to encourage LHB Directors of Primary, Community, and Mental Health Services to fight their corner on the executive side – specifically to take an active interest in comparing the funding which they actually get for mental health services with the reports submitted back by LHBs to Welsh Assembly Government!
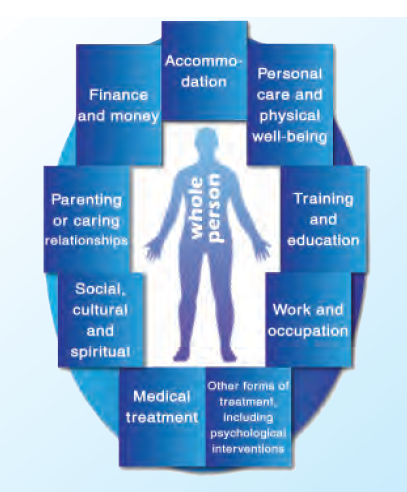
(3) The Mental Health MeasureAlthough Her Majesty signed the Measure into law late last year some of the biggest battles may still be ahead. We need to ensure that the Regulations and Code of Practice for the Measure are sufficiently prescriptive and clear. We expect consultation on the Regulations to start very shortly and Hafal intends to conduct a vigorous campaign to ensure that the prescribed content for Care and Treatment Plans (to which all secondary patients will have a legal right under Part 2 of the Measure) sets out all the “life areas” which must be addressed holistically. A late opposition amendment did set out the key areas on the face of the Measure but it will be important to ensure that these are explicitly included in the format of the plans rather than just “alluded” to in notes or guidance.
(4) BenefitsFor all that mental health patients are concerned about health and social care services it is a simple and unsurprising truth that they are most concerned about benefits. Why? Because though many or most have ambitions to achieve employment and financial independence they need the support of benefits while they work towards recovery – and those in work need the reassurance that they will be supported if they relapse.
Hafal is presently working on its response to the (UK) Government’s current review of DLA – if you’ve got any direct experience you want to share (many have already) then do let us know.
(5) The Future of Mental Health Services in WalesJust because there is a public expenditure squeeze doesn’t mean we should give up on revolutionising mental health services in Wales – though the squeeze should point us towards a cost-efficient approach obviously.
Hafal’s overwhelming sense is that change is most likely to be achieved through the initiative of patients and their families rolling up their sleeves and taking charge both of their own circumstances and, whenever practicable, of wider services. They could wait forever for the top-down approach to work and there aren’t many signs of that, though consumers should of course engage with and try to get a real dialogue going with the Mental Health Programme Board which the Assembly Government has established - even though it has no executive powers.
Shortly Hafal will announce a new campaign to encourage patients and families to empower themselves using their rights under the Measure and bringing their experience to bear on commissioning and running mental health services. Watch this space!
Keep up to date by regularly visiting
Mental Health Wales,
Hafal and our excellent
Facebook page which is alive with breaking news and snappy pictures, plus this Blog of course.
Postscript: I haven't got any personal New Year Resolutions but got off to a good start on New Year's Day by barbecuing sausages on the beach in West Wittering, Sussex, with old friend and educational consultant Nick Jarman who lives up the road. The view behind is over to Hayling Island, on the route of the British Heart Foundation's annual "Round the Harbours" bike ride - very scenic and includes two ferries (useful respite for those of only "average fitness" on the 35 mile route).